The following case is from the RENOVA trial and illustrates some caveats of stent graft treatment for VA stenosis.
A 65 YO woman with ESRD, DM, HTN, dyslipidemia, obesity presented to the access center with a dysfunctional left upper arm Brachial Basilic bridge graft placed 4 months ago. She started hemodialysis one month after the graft was placed.
Pertinent access history included high venous pressures, decreased access flows and prolonged bleeding at her cannulation sites. On exam , the AVG was pulsatile and there was a high pitched bruit at the VA. Angiogram revealed a severe stenosis at the VA and absence of other inflow or outflow stenoses. She was randomized in the RENOVA trial to the balloon PTA only arm.
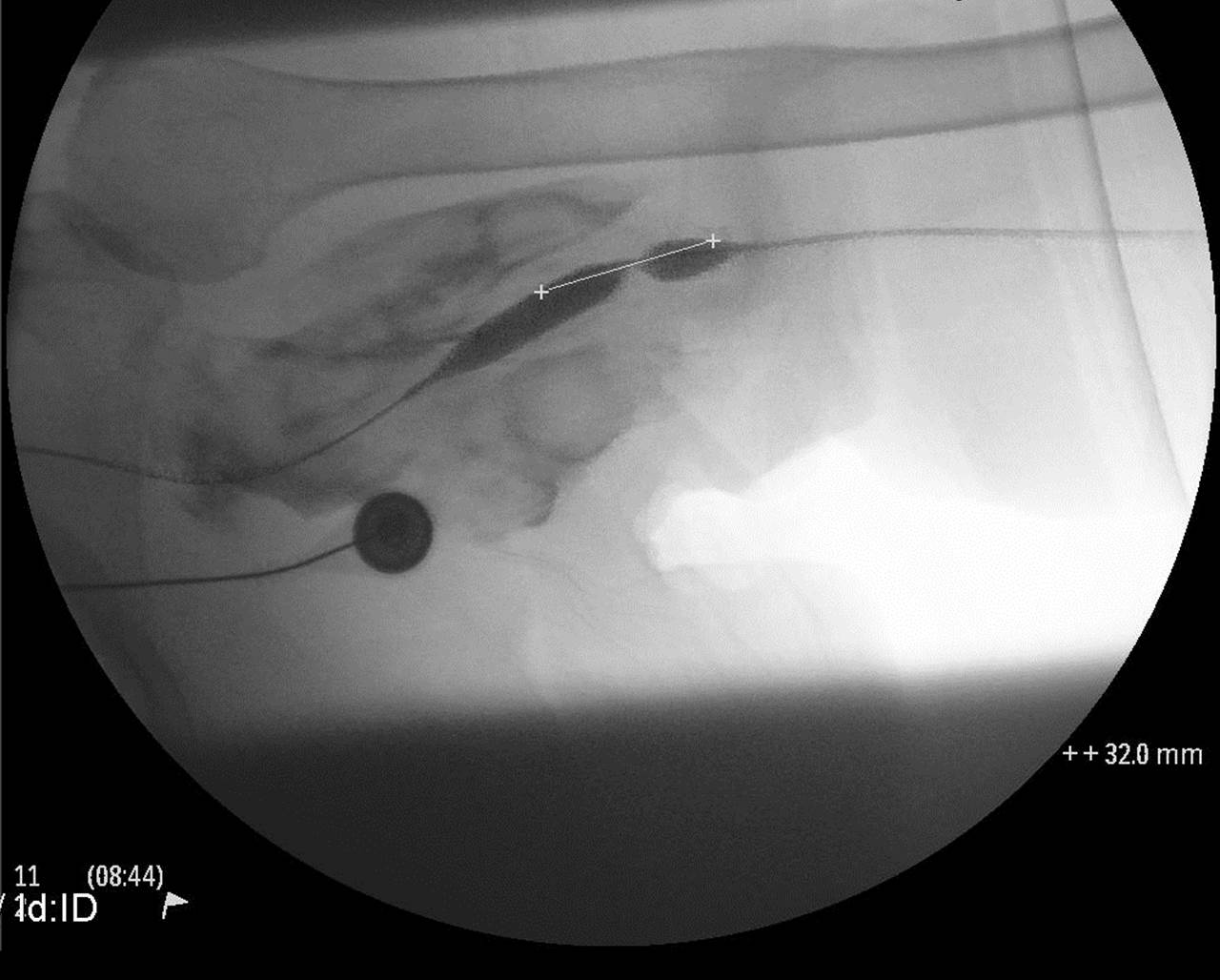
Fig 1: shows redundant graft and probably a 90 degree angle of anastomosis of graft with outflow basilic vein. The VA is 100% stenosed with retrograde flow to collaterals.
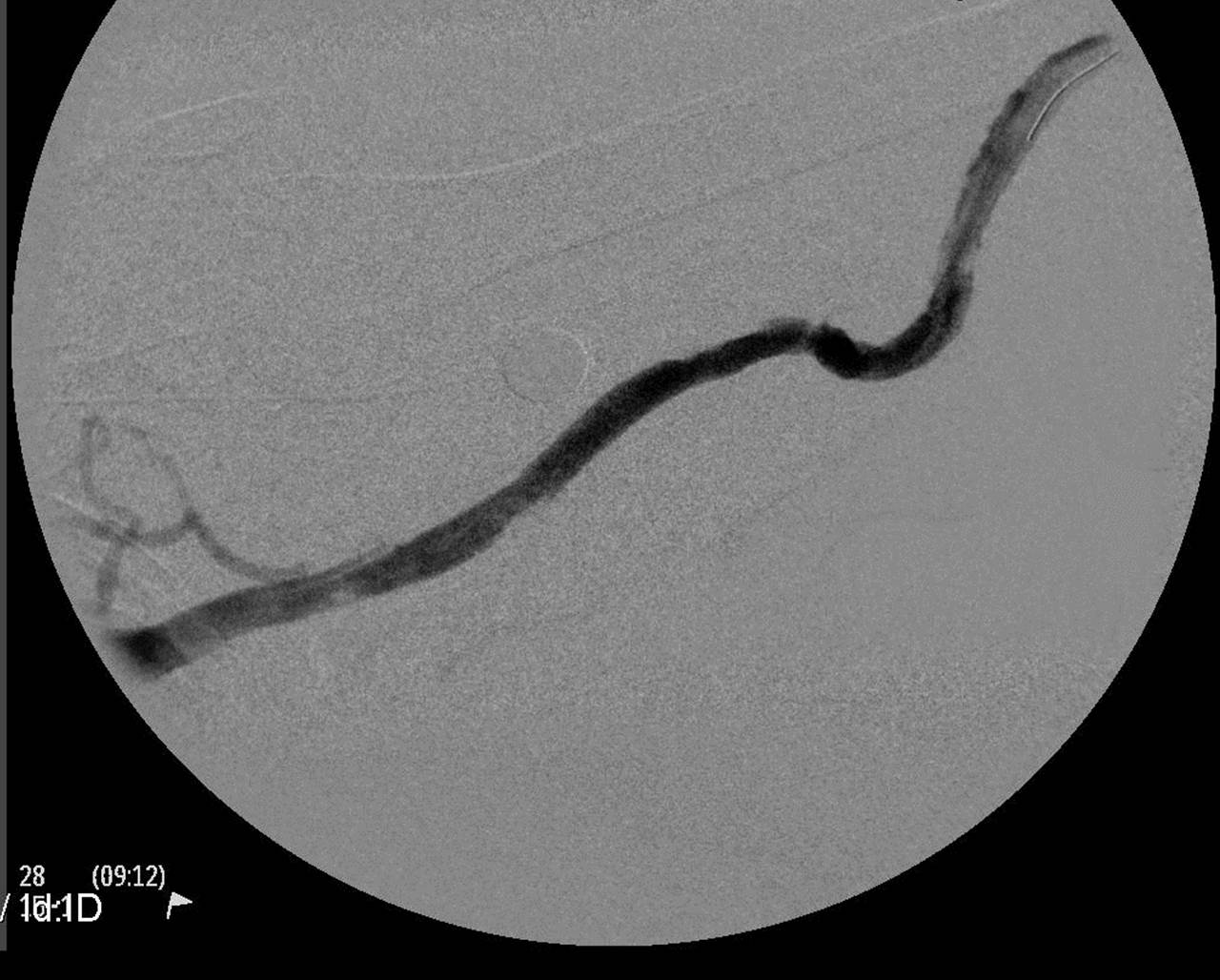
Fig 2: A wire would not cross the VA stenosis due to the acute angulation and lack of leverage using multiple guiding catheters. Therefore, the basilic vein was cannulated using ultrasound guidance at the elbow and a glidewire was threaded straight across the stenosis.
Fig 3 and 4: An 8 mm Conquest balloon was positioned across the VA occlusion and angioplastied to 30 atm. There was vascular rupture which was controlled and resolved easily with prolonged balloon angioplasty. Note the absence of retrograde and collateral flow once the true outflow path was re-established.
Fig 5: Subsequently a second glidewire was threaded across the VA from the graft access and angioplasty with the 8 mm balloon over this second wire was repeated in the VA.
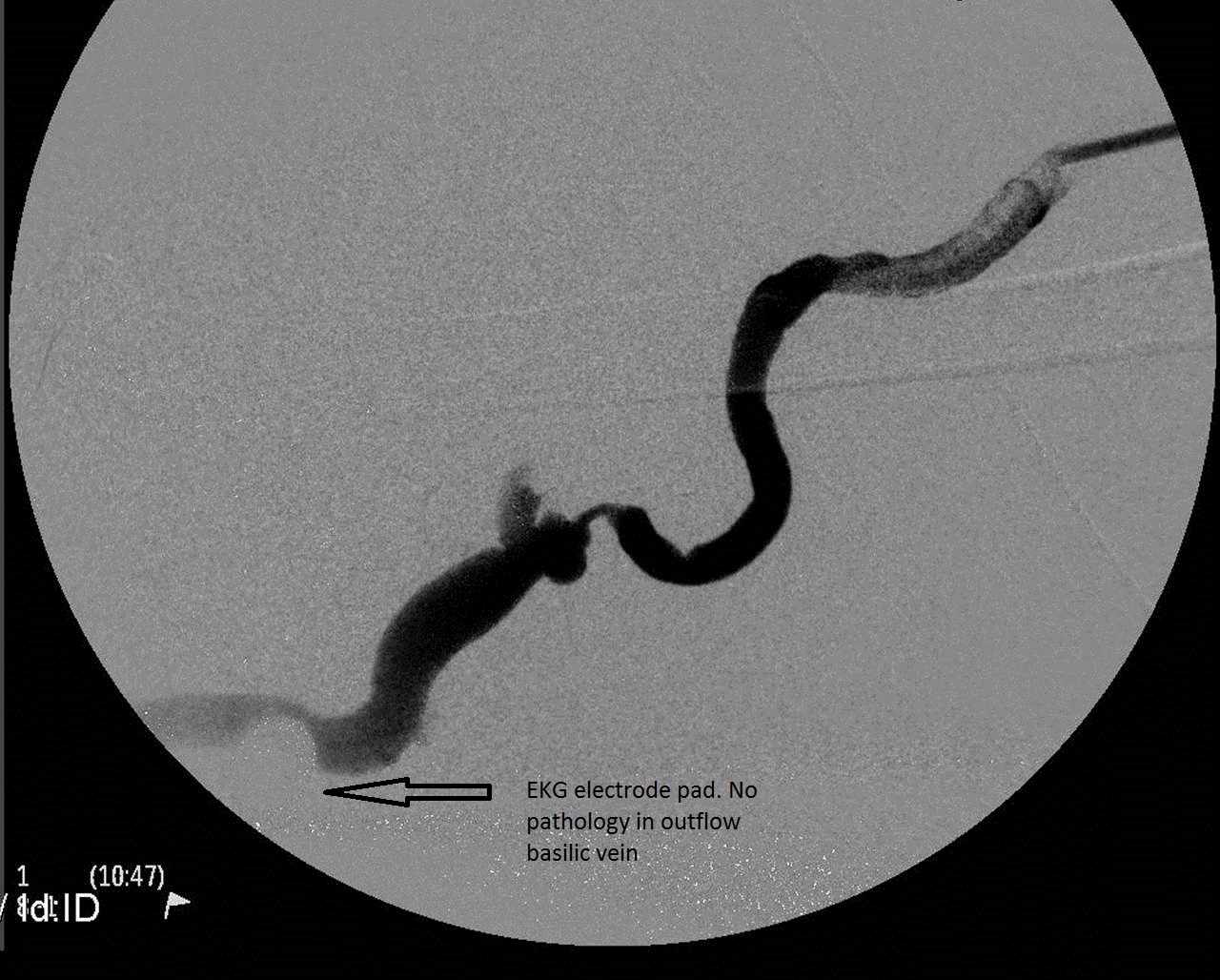
Fig 6: Post angioplasty angiogram. Outflow basilic vein is approximately 8 mm in diameter and appears healthy. The graft was a straight 6 mm ePTFE.
Fig 7: Post angioplasty angiogram with graft wire and basilic wire removed from the VA. Note the graft angulation with the VA returning.
The patient returned to the access center 2 months later with prolonged bleeding and high venous pressures.
Fig 8: The VA stenosis has reoccurred.
Fig 9: After balloon PTA with an 8 mm balloon, the VA stenosis was repaired with an 8 mm x 30 mm Flair stent graft.
This patient completed her 2 year Renova follow up without any further interventions. She continues to dialyze with this graft and is approaching her 6 year anniversary of the graft placement. Her VA has remained patent and never required further intervention since the Flair stent graft placement. She has required 4 subsequent endovascular interventions – all intragraft stenoses treated with balloon pta.
We now have 3 randomized controlled trials published in peer-reviewed journals demonstrating superior patency at the target lesion( VA) and in the access circuit using stent graft treatment vs balloon PTA for VA stenosis; the Flair pivotal trial and the Renova trial (Flair stent graft) and the Revise trial (Viabahn stent graft) . Graft VA stenosis has been recognized as a recurrent problem for 30 years and yet we have been hypnotized by the immediate cosmetic success of balloon angioplasty. Bare metal stents were tried and have never been proven any better than balloon angioplasty. These 3 stent graft trials demonstrate that we have a better tool in our tool box to treat graft VA stenosis. I highly recommend dialysis access interventionists read these published trials. One does not need to be a statistician to recognize the superior results of stent grafting VA stenosis. Much of the criticisms of this new treatment strategy has economic origins; and I agree that economics of stent graft use in the outpatient access centers are germaine. However as we transition from a fee-for-service to a bundled , accountable care , pay-for- performance paradigm of reimbursement , we need to know which tool in the tool box is going to give us the best patency. It behooves us to familiarize ourselves with how to deploy these stent graft devices ( read the IFU) and the results they can provide our patients. My experience is that instent restenosis of a stent graft in the VA is rare.
These are some caveats from the case presented.
1.She received a Flair stent graft on her second visit in the trial and required no further interventions over the 2 year follow up. She was evaluated in the balloon only ( intention- to- treat) control cohort. Therefore her excellent results which i attribute to the Flair stent VA stenosis repair actually contributed to better target and access circuit patency as primary endpoints for the balloon angioplasty control group.
2. It was fortuitous that she was randomized to the balloon only arm. A 90 degree angle of anastomosis was a contraindication to Flair stent deployment at randomization. She ended up getting stent graft treatment and my experience is that the Flair stent stiffness is an excellent "fix" for 90 degree angles at the VA. Just as the wire helped straighten the redundant portion of graft and the acute angle, i think the stent graft can help " straighten" the angle and provides theoretically more laminar flow. She had an obese upper arm and the graft has to go from superficial cannulation zone to a very deep VA; i see this frequently in obese upper arm AVGs.
3. The retrograde and collateral flow is eliminated or "jailed off" with this covered stent treatment. This was a non-issue in the trial outcomes. My experience is also that this does not cause any clinical problems. i have never seen an arm swell after a VA stent graft treatment ( forearm or upper arm graft location).
4. When does one stent graft the VA? The trials would indicate that primary treatment of VA stenosis provides best patency. Even if one does not agree and wishes to try balloon angioplasty first, i would encourage interventionists to consider stent graft treatment for those VA stenoses that reoccur in under 3 months. My dialysis patients with av graft access do not have loss of their grafts due to VA stenosis anymore ( with stent graft repair); repetitive cannulation injury and pseudo-aneurysm degeneration in the graft body are now the leading causes of graft loss and abandonment for my patients.









Posted Friday, September 9, 2016
Although I totally agree with your premise, we now have three studies that show that stent-grafts are superior to pta at the venous anastomosis, do you not think part of her problem was due to surgical technique. Firstly, it looks like the venous anastomosis was created near a valve and a branch point. Second, the 90 degree end-to-side anastomosis is obviously going cause turbulence. If you look at Dr. Ross' sutureless venous anastomosis using a hybrid graft, basically an end-to-end anastomosis with the stent-graft at the end of the graft. This technique would be helpful for obese patients as the axillary vein only has to be cannulated to create the venous anastomosis. This also may allow the axillary or basilic vein to be cannulated more proximally where it is larger. This brings me to my second thought. I am impressed that you could land a 3cm length Flair at the venous anastomosis. It also appears that the stent is over-sized for the vein where is coapts to the walls. Lastly, I have been told so much about radial force, but I find the stiffness of the Flair mostly conforms the vein to its shape instead of vice versa. I think the Flair can be detrimental based only how the vein moves with flexion-extension of the arm and shoulder. Also, under-sizing the proximal end of the stent actually improves blood flow and decreases turbulence (flow studies by Dr. Ross). As I see it, there is no real role for coapting the stent to the vessel wall. The shape of the flared-tip Flair looks nice as a selling point, but functionally it is not useful. Overall, I still want to say that I agree with Jeff. Maybe, the venous anastomosis could be angioplastied at the first intervention (although, if this patient was not in a study, one of my indications for stenting is when it takes a great deal of effort to cross the stenosis), but stent-graft placement at the venous anastomosis should occur early when there is dysfunction of the graft.
Unfortunately, I cannot get the figures to attach.