|
Posted By Gautam K. Bhanushali,
Monday, October 24, 2016
|
67 yr Caucasian male with ESRD due to Ig A nephropathy, on dialysis since July 2016, DVT left leg with pulmonary embolism in 2004, Factor V Leiden heterozygous mutation(diagnosed in 2004: on coumadin) and HTN presented in early Sep 2016 with thrombosed right upper extremity loop AVG. Thrombectomy was performed successfully. Venous anastomotic stenosis was the culprit lesion. He presented again 2 weeks later with thrombosis of the AVG. Successful thrombectomy was performed. This time, there was no significant stenotic lesion in the access. INR was between 2-3 at all visits. BP log at HD unit did not reveal hypotension episodes.
My questions are:
1) Is the recurrent AVG thrombosis due to Factor V Leiden mutation?
2) If he comes again with AVG thrombosis, would you place a catheter?
3) Should coumadin be switched to Eliquis since the risk of major bleeding with coumadin in ESRD patients is high?
This post has not been tagged.
Permalink
| Comments (10)
|
|
|
Posted By Abigail Falk,
Monday, October 24, 2016
|
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Mohammad Samih,
Sunday, October 16, 2016
|
How common is the issue of fibrin sheath around ports?
How soon after placement we see them?
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Anil K. Agarwal,
Tuesday, October 11, 2016
|
Dear Colleagues,
I want to run this interesting case by all the experts to get their insights:
A 62 year old male using a right IJ tunneled catheter for dialysis presented for a dysfunctional catheter. A preoperative examination showed good flow from both ports. However, considering the long duration of the catheter, a cathetergram was done after retracting the tip high in the neck. It showed a fibrin sheath, as expected. It was angioplastied and free flow of contrast was demonstrated. Catheter was replaced but had a 'catch' to suction of either port. Repeat cathetergram (Figure 1) suggested either a remnant of fibrin sheath or brachiocephalic vein stenosis which was angioplastied (Figure 2). The catch persisted but was intermittent. Patient left without dialysis.
At this point, I have the following questions:
Q1. What does the figure 1 show- left over sheath vs. brachiocephalic stenosis?
Q2. Does anyone have a different technique to ensure that the sheath is completely disrupted?
Q3. In either case, the tip of the catheter was in lower right atrium. Why was there resistance to suction?
The patient returned 4 days later as the catheter was again found to be 'positional' in dialysis. Repeat cathetergram (figure 3) showed a well formed sheath again (in 4 days!). This was angioplastied and catheter was replaced, but the 'catch' was again evident. The patient was convinced to get an AVG placed the next week and was sent to dialysis where it was able to be done, with only occasional alarm.
Q4. What else can be done to diagnose the issue?
Q5. Is the time to reformation of sheath proportional to the dwelling time of catheter?
Q6. Would use of antiplatelet of anticoagulant help reduce growth of sheath at all?
A week later, the patient returned for similar issues. A new IJ catheter was placed on the left side. Patient is scheduled to get an AVG placed.
 Download File (DOCX) Download File (DOCX)
This post has not been tagged.
Permalink
| Comments (15)
|
|
|
Posted By James Lin,
Thursday, October 6, 2016
Updated: Thursday, October 6, 2016
|
This is a 60y man with a RIJ tunneled catheter for many months who was referred for facial and neck swelling for 1 week. He does not have any running accesses and had a recent pneumonia with cavitary lesions which responded to therapy. I noted on exam that there was a non healing wound along the tunnel tract with no drainage and pt did not have any fever or chills. I initially planned on using a femoral approach to study the central veins and if SVC stenosis is present then move the catheter to the femoral vein, remove the chest wall cath and treating the SVC stenosis.
Then I thought it would be easier to make a cutdown over the venotomy, transecting and wiring the catheter and then evaluating the centrals via a RIJ sheath. If there is a good response to PTA of the centrals then replacing the catheter, tunneling more lateral away from the nonhealing wound over the existing tunnel.
After removing the catheter I was able to manipulate the wire through a 8Fr sheath into the IVC. It was very difficult to manipulate the wire past the mid SVC level and based on the angle and looping of the tip of the wire it was suspicious for either a high grade stenosis or thrombus. Tactile sensation suggested that it was bouncing off something and I did not think it was a stenotic lesion. I also injected through the catheter initially through a 12Fr dilator inserted into the transected catheter and there appeared to be SVC thrombus. Later injections through the 8Fr sheath revealed a massive SVC thrombus with most of the flow through the azygos vein.
I ended up putting in a femoral catheter and sending the patient to the hospital for a heparin gtt and lytic catheter by VIR.
Questions:
1) Should I have had a higher suspicion of SVC thrombus given the 1 week history of facial and neck swelling? I went into the case thinking it was a SVC stenosis with the catheter occupying the stenotic lumen.
2) If there is a suspicion of SVC thrombus would the therapy be removing the offending agent and placing the catheter elsewhere + anticoagulation +/- lytics or treating with the catheter in place. There is literature in pts with malignancies and central thrombus of leaving the offending agent (infusion catheter) in place and treating with heparin + lytics so the thrombus doesn't migrate.
3) The CT scan (picture #4) showed a massive SVC thrombus extending into the right atrium; because the thrombus did not appear to be adherent to the wall the radiologist thought it was acute/subacute. Should surgery be considered; concern is that much of the massive thrombus appears to be free floating.
4) What's the likelihood of having thrombus adherent to the catheter or fibrin sheath? This makes me concerned when we just remove catheters without any imaging. That being said I've never had a complication associated with a catheter removal. But if you are scheduled to remove a catheter and the patient has facial and neck swelling are additional studies necessary before pulling the catheter?
Pic#1 is the initial injection after transecting the catheter and injecting through the catheter pulling the catheter back so the tip is in the innominate vein. There is a fibrin sheath present.
Pic#2-3 are both injections through the 8Fr sheath in the RIJ.
Pic#4 is the CT scan of the chest with contrast.

Attached Thumbnails:
Tags:
SVC thrombus PE
Permalink
| Comments (8)
|
|
|
Posted By Abigail Falk,
Friday, September 30, 2016
|
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Felix W. Perez Ramos,
Monday, September 26, 2016
|
The patient presents to the ER with right arm and facial swelling. He has a right radiocephalic AVF. A good thrill was palpated in the AVF body, which measured approximately 12 cm. This was the area where he was cannulated for hemodyalisis.
A fistulogram was performed. The findings are illustrated above.
Fistulogram shows a complete occlusion of the cephalic vein with collateral veins that drain into the basilic vein and an 80-90% stenosis in the right innominate vein, which is the culprit lesion.
I was not able to pass the wire to the basilic vein. Because of this I did a second ultrasound-guided cannulation in the upper arm and gained access to it.
After this, I did an angioplasty using a 10 x 4 mm balloon then a 12 x 4 mm. Angiography post-dilation showed more than 30% restenosis. A 14 x 4 mm balloon was then used to dilate the vein further. Post dilation angiography showed less than 30% restenosis.
The interesting point in this case is that despite a complete occlusion of the AVF at the body there was adequate function (good kt/v,) and drainage into the basilic vein through collateral veins. The second canulation and dilation of the right inomminate vein was performed in order to decrease the swelling in the arm and face, to avoid further complications, and to continue use of this AVF. The patient has been using the AVF for 1 month following the angioplasty with no subsequent problem with the AVF and no swelling in the arm or face.
Points of interest:
1) After the central lesion was dilated, the patient has no more swelling in the arm and face and the AVF has been working properly with no complications.
2) There are physicians that could think that this AVF will not continue working adequately, but the physical exam and history of the patient suggested that the problem was not AVF, it was the central lesion, reason why I decided to do this.
3) Physical exam and medical history will help us decide what is in the best interests of the patient.
Attached Thumbnails:
This post has not been tagged.
Permalink
| Comments (16)
|
|
|
Posted By Harold R. Locay,
Friday, September 16, 2016
Updated: Saturday, September 17, 2016
|
75 y/o Hispanic male with ESRD on dialysis with a LUA brachial straight graft from 2010. He had an 8x50 Flared Flair stent placed at the venous anastomosis in 2011, had done well until 2016. He presented to our outpatient vascular access center with elevated venous pressures and prolonged bleeding. Six weeks prior he presented with the same access issues and had in-stent stenosis that underwent PTA with good result. No other pertinent medical history.
On angiogram he was found to have severe in-stent stenosis (fig. 1). PTA with a 9x4 Conquest was done with full effacement but a residual of greater than 50% was noted. A 9x50 Flared Flair was placed with 10mm overlap of the stents in the non flared section. The stent was deployed slowly but did not seem to flower well all the way back (fig. 2). A 9x4 Conquest was carefully placed to seat the stent, the stent migrated forward but was caught with the balloon (fig. 3). The stent on the balloon was pulled slightly back into the prior stent but could not be well overlapped or seated at that point as it was expanded (fig. 4). The balloon was removed and and a 10x100 Fluency stent was placed, as the Flared Flair stent continued to slowly migrate. The fluency was seated with a 10x4 Conquest and overlapped the original stent and most of the 9x50 Flared Flair stent with a space in between the two. (fig. 5). Final angiogram shows good flow (fig. 6).
Questions:
1) Should one avoid using a flared stent in a flared stent ?
2) Should one overlap more than the standard 10mm when stenting at the angle of the access (use a longer stent)?
3) Should I just snare/retrieve an unlanded stent ?
4) Should I have just pulled the stent/shaft out when I noticed the stent not flowering well (50% deployed at that point) (placed bareback) ?
Thanks
Attached Thumbnails:
This post has not been tagged.
Permalink
| Comments (5)
|
|
|
Posted By Jeffrey Hoggard,
Thursday, September 8, 2016
|
The following case is from the RENOVA trial and illustrates some caveats of stent graft treatment for VA stenosis.
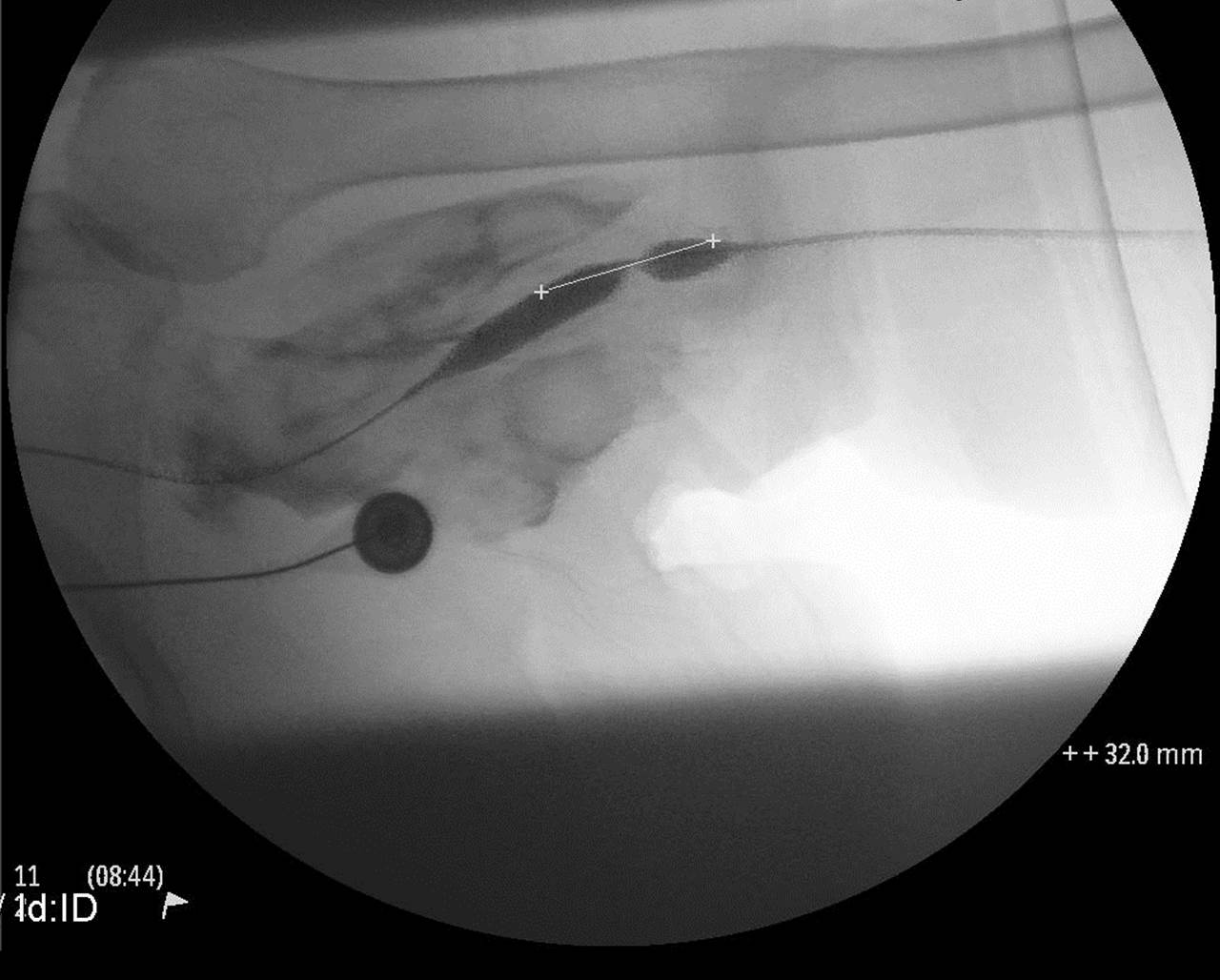
A 65 YO woman with ESRD, DM, HTN, dyslipidemia, obesity presented to the access center with a dysfunctional left upper arm Brachial Basilic bridge graft placed 4 months ago. She started hemodialysis one month after the graft was placed.
Pertinent access history included high venous pressures, decreased access flows and prolonged bleeding at her cannulation sites. On exam , the AVG was pulsatile and there was a high pitched bruit at the VA. Angiogram revealed a severe stenosis at the VA and absence of other inflow or outflow stenoses. She was randomized in the RENOVA trial to the balloon PTA only arm.
Fig 1: shows redundant graft and probably a 90 degree angle of anastomosis of graft with outflow basilic vein. The VA is 100% stenosed with retrograde flow to collaterals.
Fig 2: A wire would not cross the VA stenosis due to the acute angulation and lack of leverage using multiple guiding catheters. Therefore, the basilic vein was cannulated using ultrasound guidance at the elbow and a glidewire was threaded straight across the stenosis.
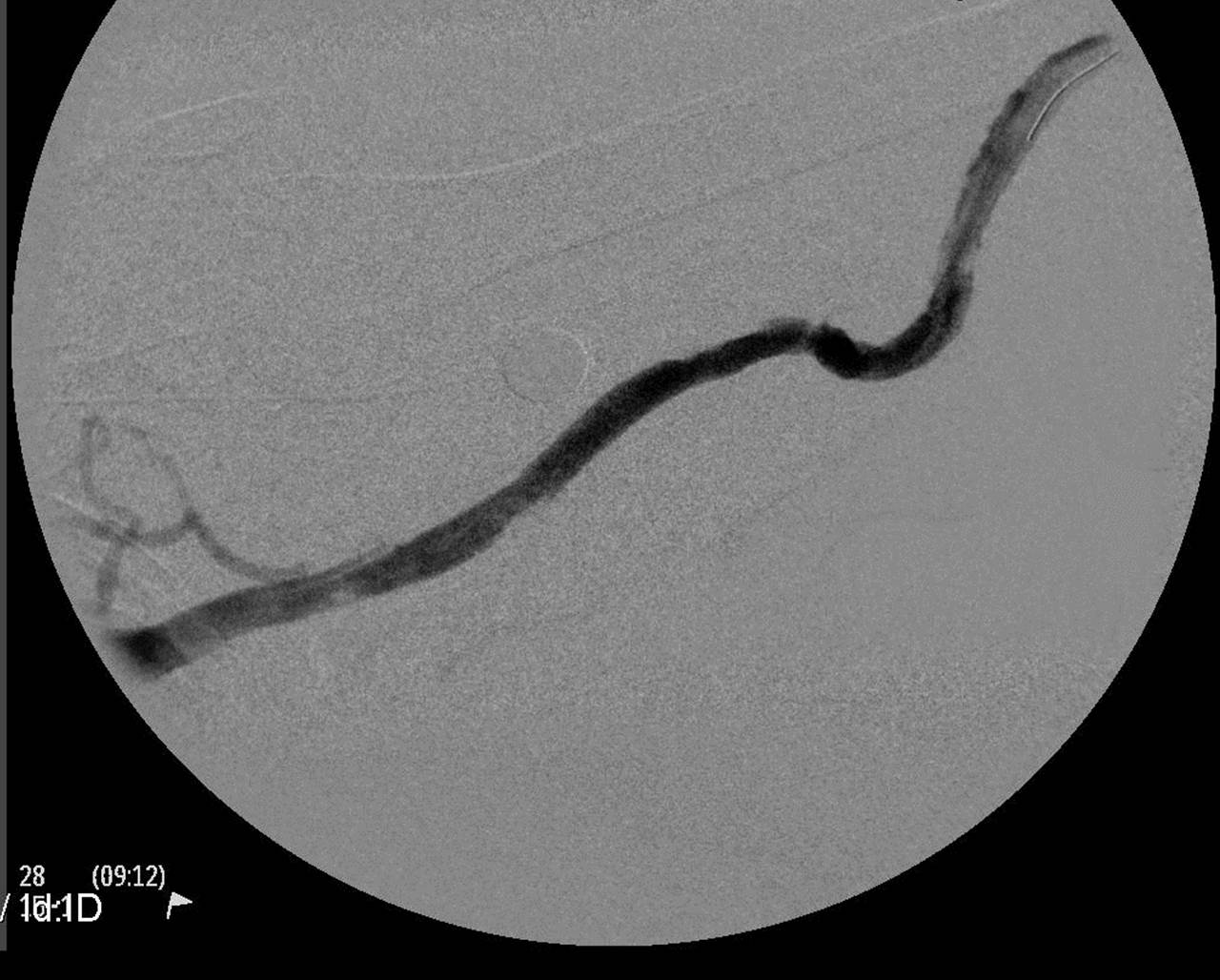
Fig 3 and 4: An 8 mm Conquest balloon was positioned across the VA occlusion and angioplastied to 30 atm. There was vascular rupture which was controlled and resolved easily with prolonged balloon angioplasty. Note the absence of retrograde and collateral flow once the true outflow path was re-established.
Fig 5: Subsequently a second glidewire was threaded across the VA from the graft access and angioplasty with the 8 mm balloon over this second wire was repeated in the VA.
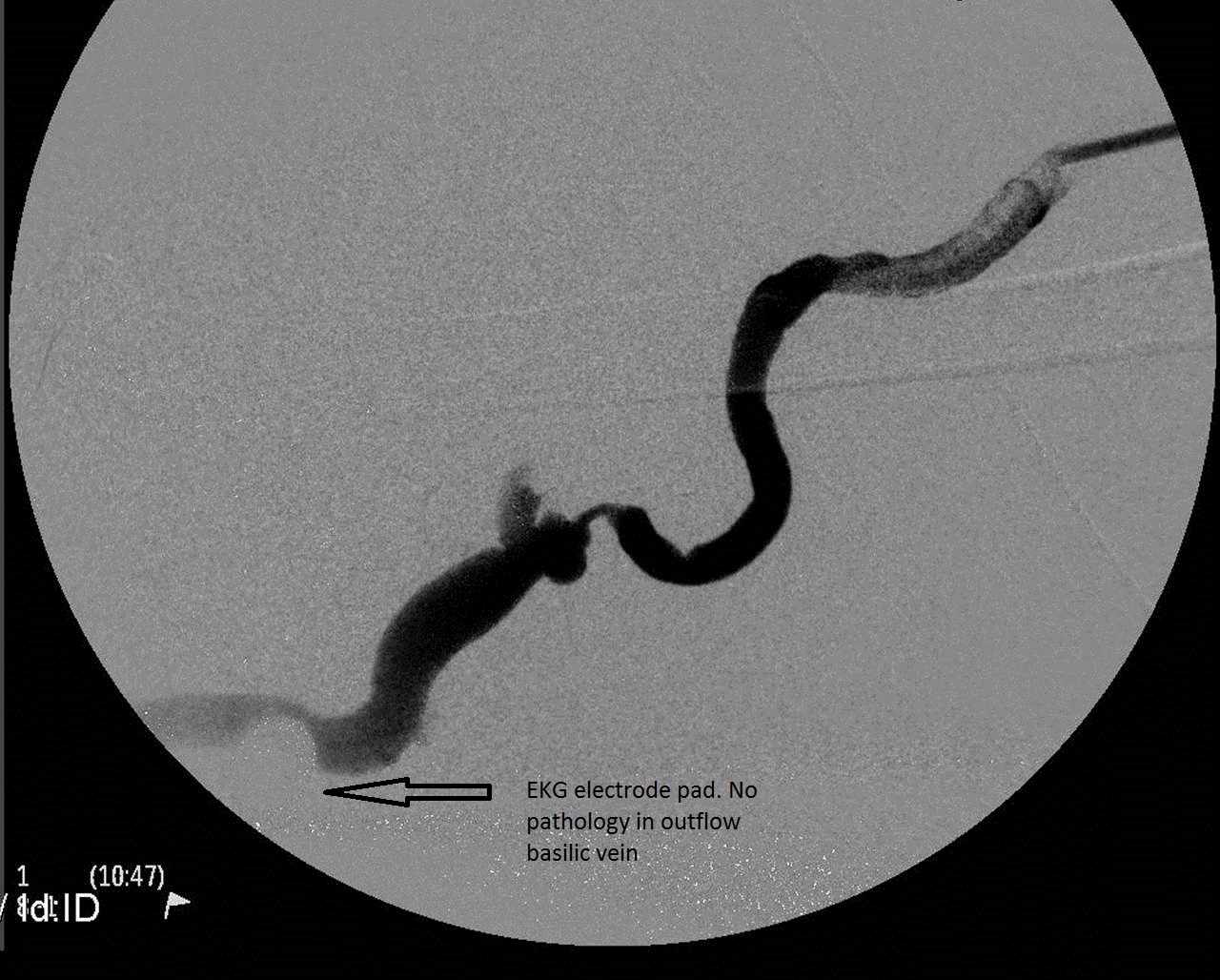
Fig 6: Post angioplasty angiogram. Outflow basilic vein is approximately 8 mm in diameter and appears healthy. The graft was a straight 6 mm ePTFE.
Fig 7: Post angioplasty angiogram with graft wire and basilic wire removed from the VA. Note the graft angulation with the VA returning.
The patient returned to the access center 2 months later with prolonged bleeding and high venous pressures.
Fig 8: The VA stenosis has reoccurred.
Fig 9: After balloon PTA with an 8 mm balloon, the VA stenosis was repaired with an 8 mm x 30 mm Flair stent graft.
This patient completed her 2 year Renova follow up without any further interventions. She continues to dialyze with this graft and is approaching her 6 year anniversary of the graft placement. Her VA has remained patent and never required further intervention since the Flair stent graft placement. She has required 4 subsequent endovascular interventions – all intragraft stenoses treated with balloon pta.
We now have 3 randomized controlled trials published in peer-reviewed journals demonstrating superior patency at the target lesion( VA) and in the access circuit using stent graft treatment vs balloon PTA for VA stenosis; the Flair pivotal trial and the Renova trial (Flair stent graft) and the Revise trial (Viabahn stent graft) . Graft VA stenosis has been recognized as a recurrent problem for 30 years and yet we have been hypnotized by the immediate cosmetic success of balloon angioplasty. Bare metal stents were tried and have never been proven any better than balloon angioplasty. These 3 stent graft trials demonstrate that we have a better tool in our tool box to treat graft VA stenosis. I highly recommend dialysis access interventionists read these published trials. One does not need to be a statistician to recognize the superior results of stent grafting VA stenosis. Much of the criticisms of this new treatment strategy has economic origins; and I agree that economics of stent graft use in the outpatient access centers are germaine. However as we transition from a fee-for-service to a bundled , accountable care , pay-for- performance paradigm of reimbursement , we need to know which tool in the tool box is going to give us the best patency. It behooves us to familiarize ourselves with how to deploy these stent graft devices ( read the IFU) and the results they can provide our patients. My experience is that instent restenosis of a stent graft in the VA is rare.
These are some caveats from the case presented.
1.She received a Flair stent graft on her second visit in the trial and required no further interventions over the 2 year follow up. She was evaluated in the balloon only ( intention- to- treat) control cohort. Therefore her excellent results which i attribute to the Flair stent VA stenosis repair actually contributed to better target and access circuit patency as primary endpoints for the balloon angioplasty control group.
2. It was fortuitous that she was randomized to the balloon only arm. A 90 degree angle of anastomosis was a contraindication to Flair stent deployment at randomization. She ended up getting stent graft treatment and my experience is that the Flair stent stiffness is an excellent "fix" for 90 degree angles at the VA. Just as the wire helped straighten the redundant portion of graft and the acute angle, i think the stent graft can help " straighten" the angle and provides theoretically more laminar flow. She had an obese upper arm and the graft has to go from superficial cannulation zone to a very deep VA; i see this frequently in obese upper arm AVGs.
3. The retrograde and collateral flow is eliminated or "jailed off" with this covered stent treatment. This was a non-issue in the trial outcomes. My experience is also that this does not cause any clinical problems. i have never seen an arm swell after a VA stent graft treatment ( forearm or upper arm graft location).
4. When does one stent graft the VA? The trials would indicate that primary treatment of VA stenosis provides best patency. Even if one does not agree and wishes to try balloon angioplasty first, i would encourage interventionists to consider stent graft treatment for those VA stenoses that reoccur in under 3 months. My dialysis patients with av graft access do not have loss of their grafts due to VA stenosis anymore ( with stent graft repair); repetitive cannulation injury and pseudo-aneurysm degeneration in the graft body are now the leading causes of graft loss and abandonment for my patients.

Attached Thumbnails:
This post has not been tagged.
Permalink
| Comments (3)
|
|
|
Posted By Deepak Sharma,
Friday, September 2, 2016
Updated: Friday, September 2, 2016
|
I recently did thrombectomy on a young patient. The graft was relatively new and clotted again after the procedure. These are the images from the second thrombectomy and I realized that I missed something first time. One image is reflux and other is on venous side. You may see it right away, otherwise I will post the answer and what we planned.

Attached Thumbnails:
Tags:
Declot
Permalink
| Comments (6)
|
|
|
Posted By Tushar J. Vachharajani,
Tuesday, August 23, 2016
|
Renal Tx in Jan 2016, Allograft working well with serum creat at 1.5 mg/dl. Now has a thrombosed HeRO. What would be an ideal treatment option to avoid risk of infective endocarditis/ bacteremia?
A) Do nothing
B) Remove the catheter portion and leave the graft intact
C) Remove the entire HeRO device
Would having information on the presence or absence of underlying central venous stenosis alter the management? Unfortunately, I have no way to get that information.
Tags:
HeRO
Permalink
| Comments (4)
|
|
|
Posted By Cutberto M. Cortes,
Friday, August 19, 2016
Updated: Friday, August 19, 2016
|
The patient is a 53 years old female with the
history of systemic arterial hypertension with 3 years of diagnosis, in
treatment with ARB losartan 50 mg PO BID. End Stage Chronic Kidney Disease with
3 years of diagnosis, with no determined cause, with instalation of IJ central
venous catheter on 13 June of 2016 and starting hemodialysis, 3 sessions per
week. No other history of importance.
Initiating with malaise, fatigue, dyspnea and
cough with sputum, 48 hours later after a hemodialysis session, initiating with
unquantified fever on 07/20/2016. She is then hospitalized for in depth
examination.
During hospitalization, it is registered low blood
oxygen saturation being as low as 61%, a chest X-Ray is taken with an image
compatible with a right basal consolidation. Relevant in Physical exploration
is in posterior Thorax presence of crackles on the right inferior area. On the
Anterior Thorax presence of a heart murmur III/VI on the tricuspid. Treatment
with moxifloxacin is initiated. Routine blood tests are taken with results in
results:
07/25/16: glucose 166 urea 128.9 creatinine 6.8
uric acid 9.1 albumin 1.87 Na 125.1 K 4.4 Ca 7.6 F 3.5 leukocites 32.12
neutrophils 26.6 Hb 6 VCM 89.5 MCHB 28.64 Platelets 167.5 procalcitonin >200.
Kidney USG: diffuse chronic changes associated
with acute inflammatory process and increased diameter of urether on the left
kidney.
Blood Cultures are taken with growth of Staph.
Aureus methicillin sensible. The IJC was removed another was placed at femoral
vein and continuing hemodialysis.
Ecocardiogram: left ventricle with 76% EF with
alterations in diastole, aortic and mitral valves normal, adhered mass on the
lateral part of the tricuspid ring and/or valve approximately 22x6 mm
suggestive of vegetation. PSAP 42 mmHg (unfortunately no images were available).
Diagnosing infective endocarditis and septic pulmonary embolism.
After an infectology consult, antibiotic
treatment was changed to imipenem/cefalotin. Also a consult for thoracic
surgery was made whom suggested a valve exchange due to the size of vegetation.
There was no requirement of vasopressors.
Finally the patient was moved to the coronary
unit and valve was exchanged. By the time patient has ben continuing
hemodialysing throught femoral catheter.
Pending the images
Download File (PPTX)
Attached Files:
Tags:
case
report
Permalink
| Comments (0)
|
|
|
Posted By Qasim Butt,
Sunday, August 14, 2016
|
38 year old Hispanic male with ESRD (presumed secondary to HTN and previous IV drug abuse) presented to our outpatient vascular center, 3 weeks post placement of right IJ tunneled catheter after initiation of dialysis. He was complaining of right sided neck swelling and tenderness for 1 week.
An ultrasound revealed a large right IJ thrombus.
Patient has no history of or predisposition to having a hypercoagulable state.
I proceeded, in our outpatient vascular center, to remove the right IJ tunneled catheter and placed a left IJ tunneled catheter. Then I directly admitted the patient to the hospital for initiation of Heparin/Coumadin.
Questions:
1) Anything wrong with my management?
2) How long would you anticoagulate with Coumadin?
3) If patient was found to have right IJ thrombus incidently and was asymptomatic, would you have done the same thing?
Tags:
right IJ
thrombus
tunneled dialysis catheter
Permalink
| Comments (17)
|
|
|
Posted By Abigail Falk,
Tuesday, August 9, 2016
|
|
Permalink
| Comments (2)
|
|
|
Posted By Abigail Falk,
Monday, August 8, 2016
|
Enjoy the articles !!!!!!!!!!!!!
https://sites.google.com/site/abigailsarticles/july-august-2016-articles
http://https//sites.google.com/site/abigailsarticles/july-august-2016-articles
Tags:
articles of interest
Permalink
| Comments (0)
|