|
Posted By Eric Ladenheim,
Friday, July 12, 2019
|
President Trump’s overall strategy of addressing the ballooning of expenditures for End Stage Renal Disease (ESRD) care by encouraging less expensive home dialysis and transplantation is brilliant but the devil is in the details. The tactics the Administration proposes to use are unnecessarily complicated and resemble a communist Chinese large scale transformative policy experiment rather than a democratic American legislative initiative.
At 4:45PM EST today on 7/11/2019 the detailed proposal was released for public inspection at https://s3.amazonaws.com/public-inspection.federalregister.gov/2019-14902.pdf. The proposed rules are 413 pages. Ironically, the authority for the regulation comes from the Obamacare Law that the Administration supports eliminating.
Here is the experiment being proposed: The USA will be divided into 306 groups of zip codes called Hospital Referral Regions. 153 Hospital Referral Regions will be randomized to provide incentives for nephrologists to refer for home dialysis (mainly peritoneal dialysis) and transplantation and 153 regions will be randomized to the status quo. The providers whose payments will be affected by the randomization will be the dialysis unit and the nephrologist. Since this is a legislative experiment rather than a clinical trial the requirement for informed consent will be waived; rather, participation will be mandatory for the providers. It is called the ESRD Treatment Choices Model (ETC Model).
When the study is concluded in 2026, the data can be analyzed to determine whether the clinical and financial outcomes are better with the payment incentives and whether the administration’s goal of increasing home dialysis and transplantation through the incentive program is being achieved. Then the incentives could be implemented systemwide.
As we well know, in recent years, CMS has been trying to reduce ESRD expenditures by reducing the payment rates for the services are were needed to maintain hemodialysis access and has run into increasingly loud resistance from providers (like myself) that performed those services and who had an opposing concentrated interest. This policy does an end-run around the HD maintenance payment conflict by incentivizing home dialysis (mainly peritoneal dialysis) and transplantation which all virtually all specialists agree is much cheaper to maintain.
That home dialysis and transplantation are less costly than in-center hemodialysis there is no doubt. Whether the clinical outcomes of home dialysis are better than the clinical outcomes of in-center dialysis are presently uncertain. In my opinion the data currently available suggests clinical outcomes are about the same. CMS proposes to resolve this uncertainty by structuring the payment reform measures as a massive nationwide prospective randomized non-blinded study that will study the effect of home dialysis/transplant payment incentives on cost and outcomes.
It is obvious that the costs of ESRD care have grown so high that something must be done or the Medicare system will be bankrupted. But America doesn’t need a grand social experiment to decide whether to incentivize less costly home dialysis and transplantation. The administration has the legal authority under the Obamacare Act to implement the proposed innovation systemwide without limiting them to randomly chosen geographic areas. I would urge that the regulations be revised before the final rule is issued making the incentives applicable throughout the America, while it monitors clinical and financial outcomes. Ultimately, the Secretary of HHS has the authority to stop the study program as soon as it is clear that money is being saved without adversely affecting clinical outcomes and make the changes permanent. I hope this is done as soon as possible.
Sincerely,
Eric
Eric Ladenheim MD
LDAC Vascular Centers
This post has not been tagged.
Permalink
| Comments (10)
|
|
|
Posted By Sun Ryoung Choi,
Friday, June 28, 2019
|
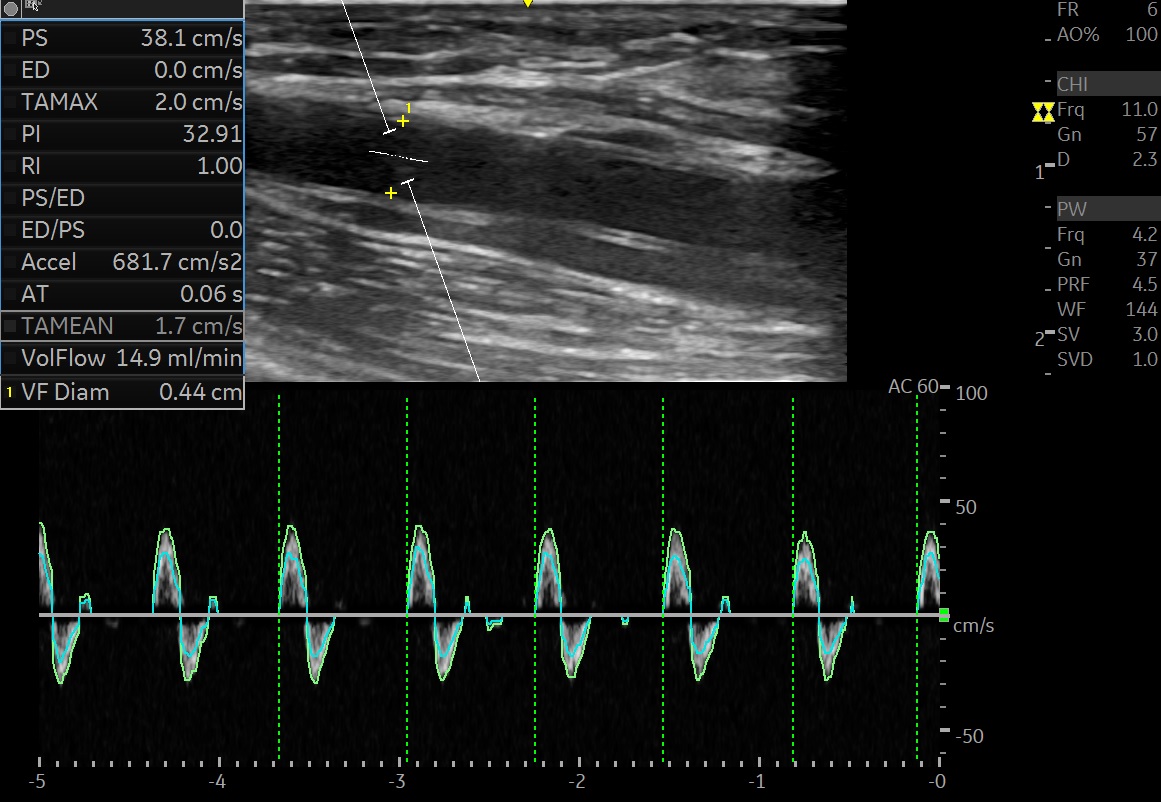
A patient on hemodialysis three times a week visited the emergency room
The patient complained of dyspnea and chest x-ray showed cardiomegaly.
Vascular ultrasound was performed on suspicion of vascular access thrombosis.
Radiocephalic fistula had no thrill.
The attached image is an ultrasound examination performed at admission.
The ultrasound waveform is thought to be somewhat different from that of general thrombosis.
In conclusion, the patient underwent pericardiocentesis as an emergency after diagnosis with
acute cardiac tamponade.
I wonder if the shape of the ultrasonic waveform of the attached file is related to the cardiac
tamponade.
Thank you.
Attached Thumbnails:
This post has not been tagged.
Permalink
| Comments (4)
|
|
|
Posted By Terry Litchfield,
Friday, April 26, 2019
|
Is anyone having issues with the tip of the Trerotola thrombectomy device separating from the basket portion? Over the last year, we have seen several of these occur and note the MAUDE database is reporting many of them. The tip is often not able to be retrieved.
The manufacturing changed to Mexico and there appears to be something happening.
And of course would want to make sure that anyone seeing a product defect should report the device failure to the manufacturer. And please report additional catheters that have the same problem.
Would love to hear if others are seeing this.
This post has not been tagged.
Permalink
| Comments (14)
|
|
|
Posted By Abigail Falk,
Monday, March 25, 2019
|
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Ryan D. Evans,
Thursday, March 21, 2019
|
Just a general technology question for the forum. I am ordering new ultrasound equipment for our surgery center. There have been recent advances allowing for hand-held US technology, such as the Sonosite iVis, Android, and Ipad devices. However, I don't see any handheld US equipment which can measure fistula flow / pulse wave doppler. I evaluate new fistulae by US to access maturation and measure flows.
Does anyone know if there are any hand-held US devices which can measure flow? Thanks.
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Gregg M. Gaylord,
Saturday, February 23, 2019
|
Has anyone hired a dialysis technician as a scrub tech for their Interventional cases? If not, what were the barriers? If so, any comments regarding state certification/scope of practice laws, training, or other caveats?
Thank You
Tags:
DIALYSIS TECHNICIAN INTERVENTIONAL SCRUB ASSISTANT
Permalink
| Comments (0)
|
|
|
Posted By Ramesh Soundararajan,
Wednesday, January 23, 2019
|
Wanted to pick your brain about a patient. Patient has hemodialysis catheter and an incidental echo and a transesophageal echo cardio gram picked up a 2 cm clot at the tip of the catheter. Blood cultures are negative but infectious diseases wants to remove the catheter. It’s working fine. Concerns about removing the catheter includes dislodgment of the 2 cm clot into the lungs. One thought is to infuse TPA to try to make the clot smaller another thought is a rather drastic step to perform open heart surgery to remove the clot. It’s possible that we have inadvertently removed such catheters and patients have done fine but having known about this problem how would you approach it. Is there any literature to support any particular action
Tags:
Clot at tip of hemodialysis catheter
Hemodialysis Cather
Permalink
| Comments (4)
|
|
|
Posted By Deborah J. Brouwer-Maier,
Friday, January 18, 2019
|
https://www.kidney.org/professionals/guidelines
Link to the National Kidney Foundation website- go to the Guidelines tab and then at the bottom of the page you can register to be a reviewer when the public review is active! Please sign-up as these guidelines will impact your local Process of Care!!!
Tags:
New KDOQI Guideline Review
Permalink
| Comments (0)
|
|
|
Posted By Deborah J. Brouwer-Maier,
Thursday, December 13, 2018
|
Ultrasound guided cannulation is slowly becoming the standard of care outside the US. See the 2017 guidelines on the use from Canada. As IN’s you routinely use ultrasound imaging. Many of you may even provide cannulation maps of a patient’s access to the dialysis unit. The Associates program at the Feb meeting will be reviewing cannulation techniques and the issue of ultrasound imaging. Wanted to get feedback on the interest in ultrasound guided cannulation or at least visualization before cannulation by your dialysis staff. Do you support the idea? Would an easy to use non-diagnostic imaging be of value to your clinics? What about cost of the device? The major adoption hurdle of training has already been disproven by Dr. Agarwal's study utilizing an easy to use simple point and see device.
thanks Debbie
 Download File (PDF) Download File (PDF)
Tags:
dialysis staff
ultrsound guided cannualtion
Permalink
| Comments (14)
|
|
|
Posted By Abigail Falk,
Monday, December 3, 2018
|
This post has not been tagged.
Permalink
| Comments (0)
|
|
|
Posted By Deborah J. Brouwer-Maier,
Monday, November 5, 2018
|
Again, ASDIN has an opportunity to lead the way in vascular access. Please help our colleague with her inquiry below.
A social worker posted on the CNSW listserv that her patient had a clotted access that has caused a lot of pain over the last few years, so we are cross-posting here. Patient now has a CVC and is getting a fistula in her other arm. The patient has swelling and pain in the arm where the fistula is clotted and has told the Social Worker that when the CVC is used it feels like her veins are being pulled out. Her surgeon has told her there isn’t a surgical option to resolve the pain she is feeling. Hate to hear of a patient having pain during each dialysis treatment. Asking for ideas to see if you have tips or suggestions.
Tags:
Pain
Permalink
| Comments (4)
|
|
|
Posted By Lindsay Fox,
Tuesday, October 30, 2018
|
Please share any feedback to the following information request from an ASDIN member:
They would like to know what policies other centers have in place in regards to a responsible person staying in the waiting room for the duration of the patients procedure. We would like to implement this, but there are a few variables. Some patients do not have anyone and rely on share a fare or other transportation options, some have someone to drop them off, and return after procedure.
This post has not been tagged.
Permalink
| Comments (1)
|
|
|
Posted By Alejandro C. Alvarez,
Thursday, October 25, 2018
|
Dear Colleagues,
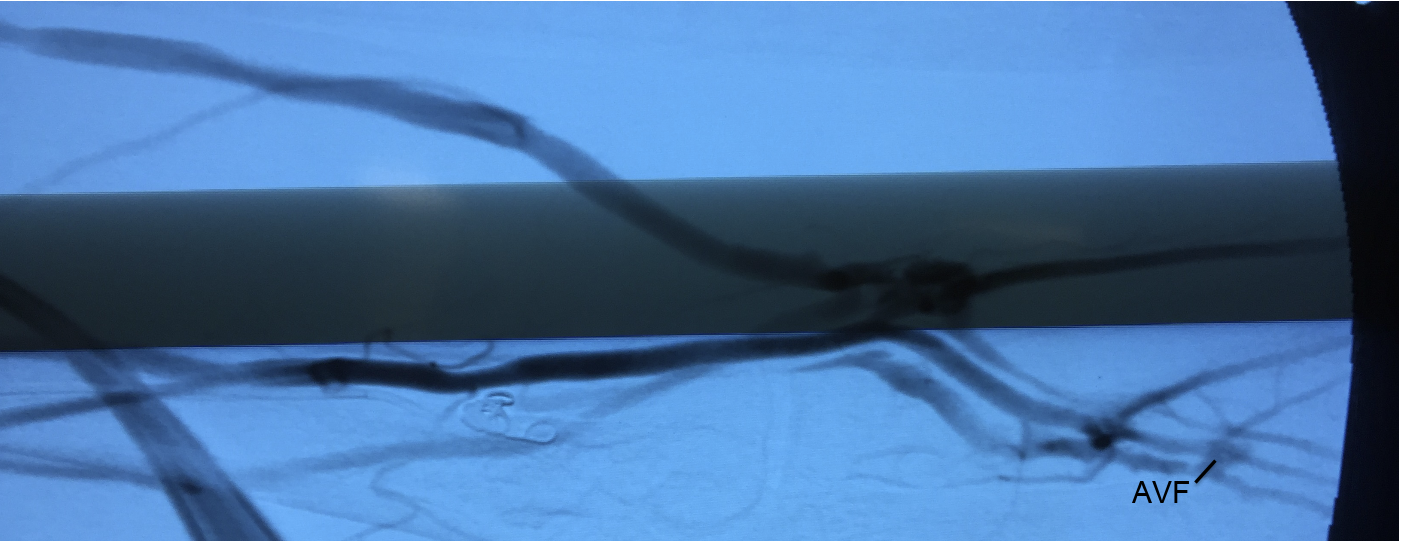
We had the Privilege to perform our first three endovascular AVF's using the wavelinQ system early this week.
All were an immediate technical success. We will follow the patients closely to the time of cannulation.
I am very grateful to my team at the VAC and the patients that put their trust on us.
Here are the most meaningful images of our very first patient - these include a the final run and blood flow volume by me two days later
The second video is the final run of the second patient.
The third is a still corresponding to the final patient.
Now we will follow them until the are ready to be accessed
Thanks,
Alejandro Alvarez
SSM VAC STL MO
Download File (MOV)
Attached Thumbnails:
Attached Files:
Tags:
AVF endovascular at SSM STL
Permalink
| Comments (2)
|
|
|
Posted By Jeffrey Hoggard,
Tuesday, October 23, 2018
|
Colleagues,
What are your methods for achieving hemostasis post sheath removal? I use a nylon suture and I write an order for my hemostasis suture be removed at the next hemodialysis session. It also serves as a reminder to the dialysis unit that this patient had something done to their access; maybe we should read the procedure note and find out if we should do something different.
One of the LDOs has adopted a policy that only allows MDs and Advanced Practitioners to remove sutures in their dialysis units. Nurses and techs have a long history of removing sutures competently. Apparently it is a liability issue.
Manual compression works but is labor intensive and takes time which is not an efficient method in a busy access center with rapid turnover. I can remember a few patients who came back to the access center who started bleeding in the car ride home. I suppose leaving the sutures for one or two weeks until the rounding MD or AP can remove the suture in the dialysis unit is safe but that does not seem ideal. Does anyone use absorbable sutures or skin glue?
Jeff Hoggard
This post has not been tagged.
Permalink
| Comments (3)
|
|
|
Posted By Administration,
Wednesday, October 10, 2018
|
ASDIN Members - We have received an inquiry from a CRNA on grafts clotting during surgery.. Please assist by responding to this post.
From Michael-Malachi Cohen CRNA, MSN
We have had at least 3 Dialysis grafts fail during surgery. The cases were at least 4 hours each and with the patient in Trendelenburg positioning. None of the cases involved direct pressure on the graft sites. If possible please supply any information, algorithm, or standard of care that you have available on intraoperative monitoring of these access sites.
Thank you for your time and effort as you look into this for our facility.
Malachi
This post has not been tagged.
Permalink
| Comments (4)
|